|
Bone Anchored Hearing Aids (BAHAs):
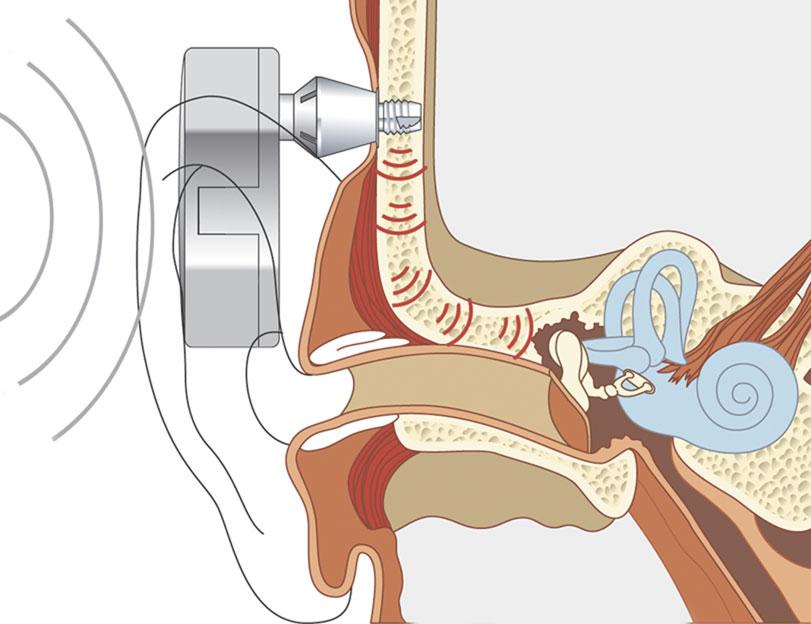
The bones of the skull are capable of transmitting sound energy to the inner ear, and this is the basis of bone conducting hearing aids and tuning fork tests. However, a traditional bone conducting aid can be uncomfortable, as it has to be pressed against the skull, and is inefficient, as transmission through scalp skin results in significant loss of energy. A bone anchored hearing aid circumvents these problems by implanting a titanium fixture and attaching a hearing aid to the fixture (Fig 1). Sound energy is amplified by the hearing aid and transmitted to the inner ear via the fixture and skull bones, bypassing the conductive loss. As there is little attenuation of energy across the skull, the contralateral cochlea is also stimulated. The choice of material is important. Titanium is particularly inert, and provided surgery is performed carefully to prevent damage to osteocytes, the titanium fixture osseointegrates with bone to provide an exceptionally strong bond, which transmits acoustic energy with minimal wastage.
In 2010 the Cochlear corporation released a new version of the BAHA fixture which hopefully will lead to improved osseointegration. Of course, the external processor, the “hearing aid” part, is constantly evolving, and the new BHA BP100 processor is Ipod and Bluetooth compatible.
Oticon have recently released the Ponto bone anchored hearing aid system, which is similar to the Cochlear BAHA system.
Fig1.Bone Anchored Hearing Aid
Indications: BAHAs are indicated for a mild to moderate conductive or mixed hearing loss not helped by conventional aids, including conventional bone conducting hearing aids. Cochlear function should be better than 45dB if a standard behind the ear BAHA is to be used, while body worn BAHAs can be used for hearing losses up to 60dB.
Children with congenital external or middle ear pathology but normal cochleas are good candidates for a BAHA, particularly if the problem is bilateral. A prosthetic auricle can be attached at the same time. Alternatively, reconstruction techniques can be considered although these are usually complex, require multiple operations and produce variable results.
Patients with chronically discharging ears, for example those with chronic suppurative otitis media or who have had mastoid surgery, and need a hearing aid, often find the hearing aid makes the ear sweaty and prone to infections and discharge. Surgical correction may not always be possible and BAHAs work well in these situations.
BAHAs produce good results in patients with otosclerosis and are increasingly being offered as a relatively safe alternative to stapedectomy.
In some cases surgery to improve hearing is possible but if the ear is the only hearing ear, patients may prefer to avoid the potential risk to hearing from middle ear surgery.
Single sided deafness: As sound energy is transmitted across the skull bones to both cochleas, a BAHA can be used as an alternative to a CROS (Contralateral Routing of Signal) aid. CROS aids require sound from the deaf side to be fed into the good ear, and patients complain about the good ear being blocked. A BAHA avoids occlusion of the good ear, and about two thirds of patients with a BAHA for single sided deafness report improved hearing from the deaf side, localization of sound and hearing in background noise. Currently for total loss of hearing in one ear with good hearing in the contralateral ear, a BAHA or CROS aid are the only realistic treatments.
Disadvantages:
Cost. The cost of the BAHA and implantable kit is approximately £5000, and there are additional costs for hospital, surgeon and anaesthetists fees. Some insurance companies cover the costs fully, others cover only the cost of surgery, while some do not cover any of the costs. There may be additional ongoing costs for repairs, treatment of minor skin infections etc.
Surgery is required to implant the device, although this can be under local or general anaesthetic, and can usually be carried out as a single stage procedure. As the middle ear is not entered, the risks of middle ear surgery such as damage to hearing or the facial nerve do not apply.
Minor skin infections can occur around the abutment, and daily cleaning around the abutment is required.
Trauma may damage or loosen the fixture, particularly in children, and replacement may be required.
BAHAs are a safe and effective treatment for moderate conductive and mixed losses.
|
